The success rate of non-surgical root canal treatment is high, however, inadequate obturation and inability to seal anatomical complexities can play a role in the long-term success of endodontic treatment. Traditional root canal sealers tend to shrink or wash-out—BioRoot™ Flow is a mineralbased, tricalcium silicate sealer with bioactive properties which slightly expands upon setting and has a high pH, therefore providing antimicrobial properties.
Methods
The patient presented with a previously treated tooth #30 (mandibular right first molar) with apical periodontitis, and unobturated disto-lingual (DL) and middle mesial (MM) canals. The case was re-treated by the author and at the one-year follow-up, excellent apical healing had occurred.
Discussion
The success of root canal re-treatment requires that bacteria be eradicated from the canals, and the canals be sealed long-term. Active biosilicate technology in BioRoot™ Flow allows for antimicrobial effects and apical bone healing.
Conclusion
BioRoot™ Flow played a critical role in the success of the root canal re-treatment of this case, with excellent sealing and antimicrobial properties.
CASE REPORT
Clinical signs and symptoms
The patient presented in June 2022 for a consultation. Her dentist and hygienist recently noted periapical radiolucencies associated with tooth #30 (mandibular right first molar) on a full mouth set of radiographs. The patient was asymptomatic, but since she was told she may have “infection”, she presented to the author for an endodontic consultation.
The dental history was remarkable for root canal treatment of tooth #30 being performed in 2016. No follow-up radiographs had been taken since 2017.
Diagnosis
An extra-oral and intra-oral examination were performed. There was no lymphadenopathy, swelling, erythema, or a sinus tract. Tooth #30 was non-sensitive to percussion and palpation, had physiologic mobility, a 4 mm mid-buccal probing (all others were <4 mm), and was non-responsive to cold due to previous endodontic treatment. The tooth was currently restored with a porcelainfused to metal (PFM) crown with composite in the access cavity.
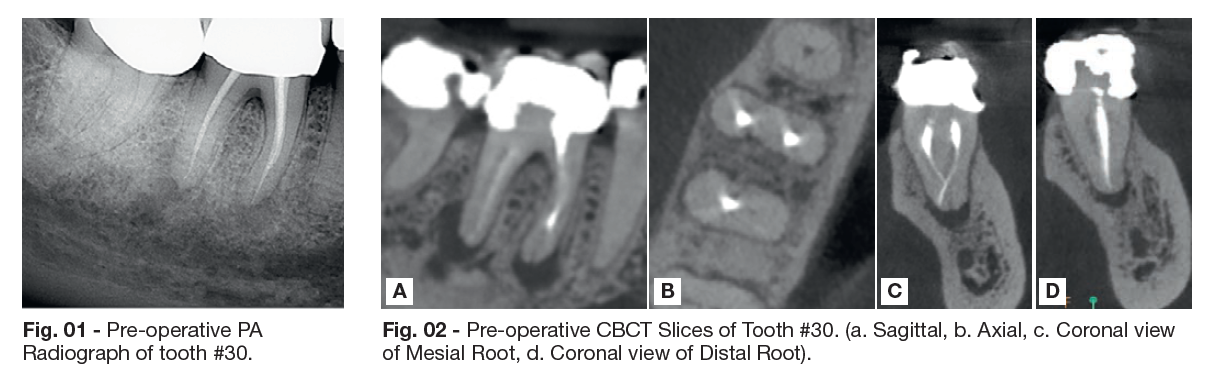
For radiographic diagnosis, a periapical (PA) radiograph (Fig. 01) and limited field of view CBCT were exposed (Fig. 02a-d). The previous endodontic treatment included obturation of three (3) canals, with inadequate density of obturation in the apical 1/3 of the M and D roots. Apical radiolucencies were present at the mesial (3x3 mm) and distal (3x5 mm) apices. The CBCT (Fig. 02a-d) confirmed an unobturated distolingual (DL) canal and possible middle mesial (MM) canal; the coronal CBCT slice of the mesial root (Fig. 02 c) also suggests an apical delta, rather than a single apical foramen. No signs of cracks or fractures were visible.
Procedure and treatment
Two (2) days after the consultation appointment, the patient presented for non-surgical root canal re-treatment of tooth #30. Informed consent was reviewed and obtained. Local anesthetic and rubber dam isolation were performed. The access cavity was opened to give access to the previously obturated, as well as the untreated canals. Hand and rotary instruments, along with solvent, were used to remove existing gutta percha in the MB, ML, and DB canals. The DL and MM canals were also identified and instrumented. The electronic apex locator was used to determine working lengths for each canal. Patency was obtained on all canals. The canals and chamber were irrigated with 6% NaOCl (30-gauge, side-vented needle).
Gentle Wave irrigation was utilized as an adjunct to traditional irrigation. Gutta percha was fitted in each canal and a master cone radiograph was exposed to ensure appropriate fit. The canals were dried, and BioRoot™ Flow sealer was injected to mid-root of all canals, using the luer-lock tip provided by the manufacturer. The tip of the BioRoot™ Flow syringe was then removed and the gutta percha cones were coated by inserting them carefully into the remaining sealer in the tip of the syringe. This allows to save on sealer but also to fully obturate. Once the cones were coated, they were seated to length. A heated plugger was used to sear gutta percha at orifice level, followed by compaction. The access was then restored.
A post-operative PA radiograph was exposed (Fig. 03) and home care instructions were reviewed.
The next day, the patient was called on the telephone to see if she had any questions or concerns. She said she was doing well, but was mildly sore, and had taken ibuprofen one time.
Follow up
6-month Follow-up (January 2023): The patient returned for a routine follow-up appointment and stated, “I’m doing well!” A clinical exam was performed, and the mid-buccal probing had returned to a normal depth of <4 mm. All teeth in the quadrant were non-sensitive to percussion and palpation; there were no signs of erythema, swelling, or a sinus tract. The patient consented to a PA radiograph and limited field of view CBCT scan. The PA radiograph (Fig. 04) shows a small mesial sealer puff; the apical radiolucencies associated with the mesial and distal roots have decreased in size from June 2022 (comparison of Fig. 01 and Fig. 04).
The CBCT (Fig. 05) shows a significant decrease in the size of the apical lesions, demonstrating excellent healing at the 6-month mark. Recommendation: Follow-up in 6 months, since healing is expected to be near completion at the 12-month mark.
12-month Follow-up (June 2023): The patient states “I’m doing well. Just here for a routine check.” The patient is asymptomatic and probing depths were all <4 mm around #30. Tooth #30 was non-sensitive to percussion and palpation, with physiologic mobility. The patient consented to PA radiographs (Fig. 06 a-b)) and a limited field of view CBCT scan (Fig. 07 a-c). The PA radiographs (Fig. 06 a-b) show signs of healing at both the mesial and distal apices.
The CBCT (Fig. 07 a) highlights the obturation of the middle mesial canal, and the convergence/joining of the DB and DL canals. The M and D coronal views (Fig. 07 b-c) confirm apical healing of both roots Clinical and radiographic findings indicate #30 as healed. No further follow-up is required unless the patient or her dentist notice changes in clinical or radiographic signs/symptoms.
DISCUSSION
The goal of endodontic treatment is to create an environment where apical periodontitis can heal. Studies show that “… failure in endodontic treatments is associated with the low quality of root canal fillings” (Marconi, et al.). Many clinicians desire to improve their obturation techniques, since this can minimize the chance of failure and re-infection. A systematic review in 2022 found that there are “… no differences in the success rate of primary non-surgical endodontic treatments when the cold lateral compaction technique and other obturation techniques are performed. Further welldesigned studies are still necessary.” (Marconi, et al.). Therefore, clinicians can choose from a variety of obturation techniques, and can select the technique that works best in their hands. In this case study, a single-cone/hydraulic condensation technique was utilized. This technique is generally considered to be a “cold” technique since heat is only applied at the orifice level to remove excess gutta percha. Cold techniques are mandatory with some sealers since heat application can alter the sealer’s setting process. This is not the case with BioRoot™ Flow, since the sealer sets in the canal using the inherent moisture and humidity of the root dentin; this means that warm and cold techniques are all acceptable for use with this sealer.
In addition, it is known that approximately 35% of the root canal walls are un-touched by endodontic instruments (Peters, et al.). This means that endodontic success relies on a combination of antimicrobial treatments (such as irrigants and sealers), and obturation, to minimize the space where bacteria can survive and multiply.
BioRoot™ Flow is unique because it is highly pure and biocompatible; this allowed the small sealer puff on the mesialroot of this case to be well-accepted by the body.
In addition, BioRoot™ Flow slightly expands upon setting, which helps to block dentinal tubules where bacteria may survive and multiply. Finally, the high pH of the sealer contributed to the anti-microbial efforts of the provider/author. BioRoot™ Flow builds on the legacy of BioRoot™ RCS, which was introduced in 2016. BioRoot™ Flow became available in 2022, making active biosilicate technology easier to use in a syringable form. Studies show that “[c]alcium silicates-based sealers promote apical healing, possess antibacterial activity, and bond to tooth structure. Their biological properties depend on… a hydration reaction followed by a precipitation reaction of calcium phosphate and formation of hydroxyapatite” (Zavattini, et al). These properties have empowered clinicians to achieve high quality endodontic results for their patients.
Septodont’s BioRoot™ Flow builds on the legacy of BioRoot™ RCS, which is known for being non-cytotoxic, and induces angiogenesis and osteogenic growth (Camps, et al.). In this case study, BioRoot™ Flow played a critical role in the success of root canal re-treatment, with excellent sealing and antimicrobial properties.