
Glass-Fibre-Reinforced Composites as a Core Build-up in Minimally Invasive Endodontics
Even though dentistry is nowadays focusing more and more on prevention, there is still a considerable amount of patients with extensive caries lesions in need of endodontic treatment. When the damage has already occurred, it's important to treat the lesion in a minimally invasive way. Preserving the cervical dentine is of utmost importance here, as maintaining a ferrule is necessary for a good prognosis of the restorative treatment.
Since the introduction of microscopes and NiTi files in dentistry, preservation of the cervical dentine has become more simple and predictable.
Several options exist for the post-endodontic treatment [1]: the treatment plan depends on the remaining tooth structure, wall thickness and the total cavity size.
Heavily damaged teeth often end up in a restorative cycle, with increasingly larger restorations after the original fractured and endodontic retreatments, the prognosis of the tooth becoming more and more challenging each time. Hence, it's important to implement a correct treatment plan to preserve the teeth not only in the short term, but to avoid catastrophic failures that compromise the long-term survival.
The first step is to preserve the tooth tissue, especially in the cervical part of the crown. Preparation designs based on root canal orientation allow for very conservative access cavities and give a better restorable prognosis in fracture cases [2].
At the restorative side, fibre-reinforced composites (FRC) can be used to reinforce the cavity. Several studies have highlighted that the fracture pattern and load-bearing capacities of large cavities restored with FRC was more favourable compared to those restored with conventional direct composites [3,4]. Hence, FRC become a promising solution for post-endodontic treatment, mostly in cases with conservative access.
One of the suitable indications for FRC is the endodontically treated premolar with one big orifice and one large oval canal or deep furcation (Figs. 1-4). In such cases, an FRC can be placed as a Nayyar's core modification [5] without preparing the orifice part with Gates or Largos. The restoration can be finished as usual, directly with a conventional composite.
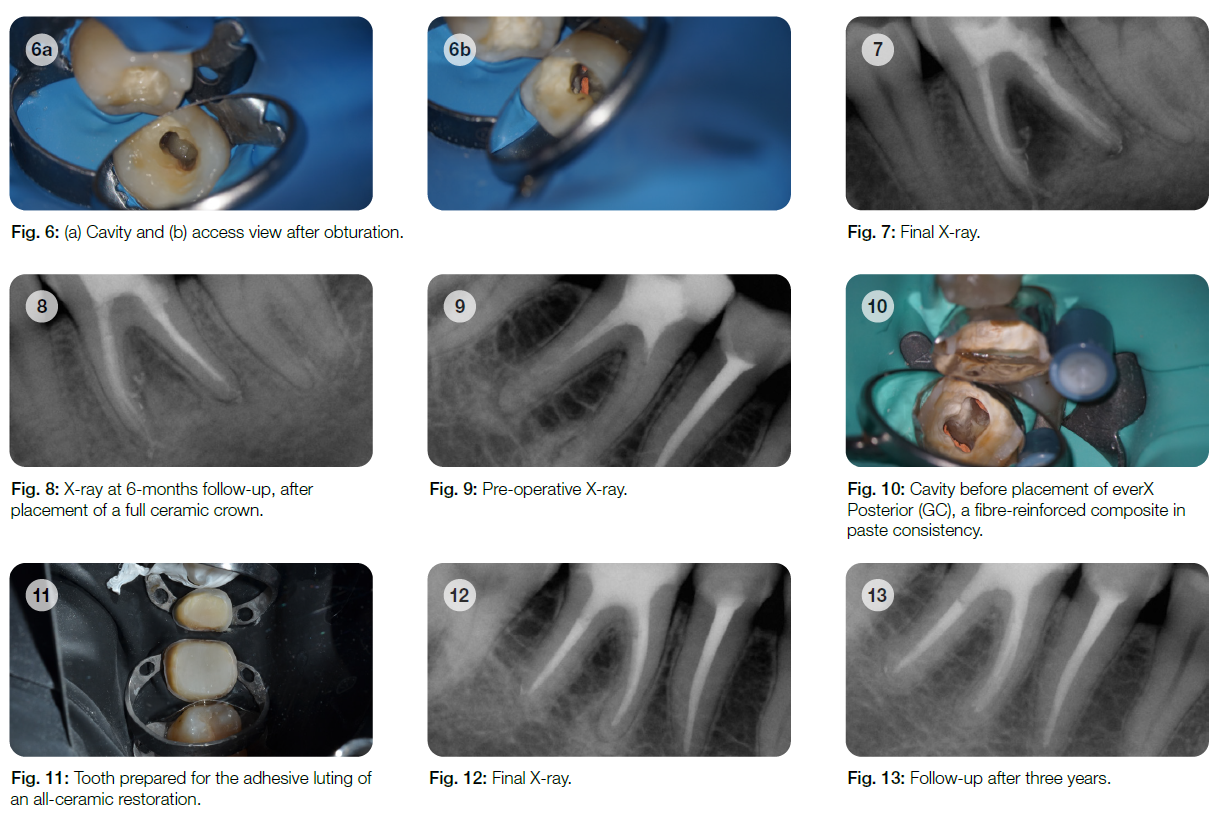
Endodontically treated molars with conservative access do not require a post. Of course, the final treatment does not only depend on the access type, but also on the size and depth of the cavity. Here, FRC have also proven their worth in complicated cases with internal resorptions (Figs. 5-8).
Even when the endodontic treatment is finished with an indirect restoration (a crown, onlay or overlay), FRC can be used for core build-ups such as a Nayyar's core. This will be mostly indicated in retreatment cases, were the orifice part of the canal had already been prepared (Figs. 9-13).

EverX Posterior™ and everX Flow™ are excellent options to restore the core of endodontically treated teeth. Together with the preservation of cervical dentine, they are part of a strategy to increase the longevity of the post-endodontic restorative treatment.


References
1. Zarow M, Ramírez-Sebastià, Paolone G, de Ribot Porta J, Mora J, Espona J, Durán-Sindreu F, Roig M. A new classification system for the restoration of root filled teeth. Int Endod J. 2018; 51(3):318-334.
2. Özyürek T, Ülker Ö, Özsezer Demiryürek E, Yilmaz F. The Effects of Endodontic Access Cavity Preparation Design on the Fracture Strength of Endodontically Treated Teeth: Traditional Versus Conservative Preparation. J Endod. 2018; 44(5):800-805.
3. Garoushi S, Sungur S, Boz Y, Ozkan P, Vallittu PK, Uctasli S, Lassila L. Influence of short-fiber composite base on fracture behavior of direct and indirect restorations. Clin Oral Investig. 2021 Jan 8 (Online ahead of print).
4. Geerts G, Pitout E, Visser H. Fracture resistance of endodontically treated premolars with fibre-reinforced composite restorations. Eur J Prosthodont Restor Dent. 2011; 19(1):25-31.
5. Nayyar A, Walton RE, Leonard LA. An amalgam coronal-radicular dowel and core technique for endodontically treated posterior teeth. J Prosthet Dent. 1980; 43(5):511-5.