In mid-2023, leading up to and then following the release in December 2023 of the new Australian Standard 5369 on reprocessing reusable medical devices, I had been working on updating the ADA’s Infection Prevention and Control Guidelines for what would become their May 2024 fifth edition. This was part of my role of serving as the editor of those Guidelines, something I have done since 2010. Given that the new standard placed considerable role on local facility risk assessments, I had been undertaking some deep analysis work to identify areas of failure that could occur in a dental practice that was reprocessing instruments on site. From looking at the literature and also from reviewing my own experience auditing dental practices, it became clear that the topic of ultrasonic cleaning was not as well understood by end users as it should be. It is also one where I felt that there was considerable work yet to do.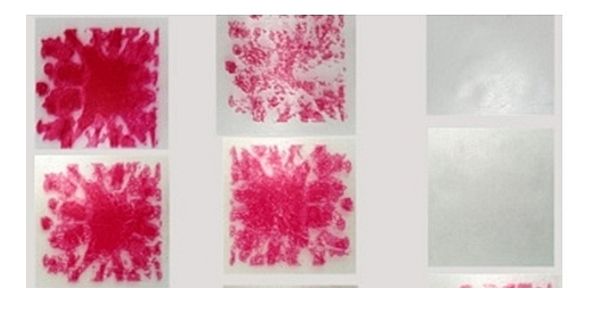
I saw this work as consisting of several tasks. The first of these was to create a structured tool for assessing all of the risks associated with improper ultrasonic cleaning. This became part of an ADA member-only tool on failure mode effect analysis, which will be released later in 2025.
The second area of work was to recreate a number of scenarios in my own lab to test their impact. I did this by purchasing a new ultrasonic cleaner that had temperature control for the fluid, so that I could start to explore the effects of temperature as well as other important variables such as water hardness. I had already collected tap water samples from over 40 locations across Australia, and my analysis of those water samples for hardness and other characteristics highlighted that there was going to be an impact of water hardness on ultrasonic cleaning in many regions of Australia.
The third area of work was then to consider the performance of different types of cleaning detergents used for ultrasonic cleaning, especially those sold for use in dental and medical practice environments. As I began to talk more about the topic of variables in ultrasonic cleaning in my various lectures and courses, the response from those attending these reinforced to me the need for a deeper dive into what was happening in the ultrasonic cleaning process.
I was already quite familiar with the cavitation processes that occur during ultrasonic cleaning, having used this concept for almost 20 years in various research protocols, including testing different fluid agitation technologies and different cleaning detergent fluids. The missing thing in the literature was a structured assessment of how different products perform, as factors such as concentration, time, and temperature are varied. Likewise, much of the literature on reprocessing in the large hospital environment using ultrasonic cleaning has showed more emphasis on enzymatic agents. Typically, in dentistry, the use of enzymatic agents has been limited to specific protocols, such as those used for rotary Ni-Ti endodontic files. My research group have conducted multiple studies using enzymatic agents. We had found that the degree of difficulty was increased by allowing residues and bioburden to dry overnight or longer on instruments before ultrasonic cleaning. These studies showed to me the value of enzymatic agents that could attack and break down organic bioburden.
Thinking about these types of issues drove my interest in developing an investigation that could help address the gap in the literature around the differential performance of products used with the ultrasonic cleaning of dental instruments. Such a study would need to have a very robust challenge for the cleaning process, one which was readily available and highly reproducible. Having looked into different types of natural and artificial soils, one feature which was attractive was a standardised challenge which was highly coloured, making the test soil strips amendable to digital image analysis, so that the results could be quantified. I had first used this type of area-based image analysis approach more than 35 years ago while working in North America on the performance of alcohol-based hand gels, and today the available software to perform it is much more powerful and user-friendly than it was all those years ago.
So having found an appropriate challenge and a suitable quantification method, the next thing was to design a series of experiments to explore independently the different key variables. One thing that becomes immediately obvious is that some products do not give a fixed dilution rate, but instead give a range that the user may choose from. Typically, product information is not particularly useful in guiding the choice of dilution. I had found during clinic audits that most practices use the greatest dilution because that was the most economical. Thus, it was important to look at products used in a comparable way, matching like for like, e.g. at the recommended highest and lowest dilution across different products. It was logical to test products at different water temperatures and for different exposure times. I had found during audits that many staff were not aware that warm water should be used, so it was important to test both cold tap water and warm water. Likewise, given the common occurrence of hard water across Australia, it was important to look at the influence of water hardness as a further factor in the mix of variables.
The final part of experimental design was to choose a range of different commercial products, some which operate purely by chemical action, and others that have one or more enzymes. This would give an opportunity to see the difference in performance according to the fundamental mechanisms of action of the product.
Our research group was fortunate in having several enthusiastic young researchers who had expertise in microbiology who were keen on pursuing this type of project, and they have the patience to run the numerous repeat cycles testing the different conditions for the standardised test strip. The next revolution was to progress onto using a standard soil that included a fluorescent dye tracer, and allow this soil to dry overnight onto actual dental instruments. Using appropriate image analysis, the amount of remaining soil could then be measured very accurately, and the results used to compare the relative performance of different products.
In the final analysis, it is important to know the conditions that are required to achieve a high level of performance. A product that has a less-than-optimal formulation will not remove much soil, and will work slowly. This will require repeated cleaning cycles to achieve a visibly clean item, which impacts upon the turnover efficiency of instruments, as well as on staff time. A highly effective product will clean quickly and will reliably give visibly clean items in a shorter time period. This optimises the dynamics of instrument turnover, and makes staff time more efficient, since repeated cleaning cycles are not needed. Thinking purely from a financial aspect, getting to the desired result sooner not only saves staff time, but it also means that a smaller inventory of instruments is needed to keep the clinic operating smoothly. This type of “time and motion” thinking should be a part of how people assess their own ultrasonic cleaning product choice. It is far too simplistic to simply work out the cost per litre of the cleaning product. One has to consider the dilution rate and the effectiveness of the product.
At the end of the day, what seems like a straightforward procedure done in the back-of-house reprocessing areas in thousands of dental clinics around the country needs a lot more attention. If items are coming out with contamination still present, those are not fit to proceed to steam sterilisation. Ultrasonic cleaning is certainly one of the most critical parts of the entire journey of reprocessing. For many dental clinics, it will be a major weak link in the chain of events which staff need to undertake to make dental care safe for patients.
To read further research and editorials click here
See our blog post about Henry Schein's Optizyme Ultra D: An Advanced Tool for Dentistry
Author:

Emeritus Professor Laurence J. Walsh AO
BDSc(Hons), PhD, DDSc, GCEd, FRACDS, FFOMP(RCPA), FDFTEd(RCS Edin), FICD, FADI, FPFA, FIADFE
School of Dentistry, The University of Queensland